
When COVID-19 first reached Australia, Federal and State Governments implemented a series of behavioural control measures, including physical distancing and isolation/quarantine to reduce virus transmission. Covasim was used to provide government with information about the likely impact of relaxing various control measures, and the time required to monitor the impact of relaxing these measures.
The model has since been used to assess testing strategies, school policies, and the possible epidemic trajectories of new variants of concern.
Burnet’s COVID-19 mathematical modelling was commissioned by the Victorian Government to inform the Victorian Roadmap.
The Roadmap was developed based on expert modelling from the Burnet Institute and is set against COVID-19 thresholds including hospitalisation rates, and the vaccination targets already set out in the National Plan to transition Australia’s National COVID-19 Response.
“The modelling helped the Victorian public health teams get a picture of what our hospitalisation rates could look like while cases are still rising and develop trigger points to indicate if the system is becoming overstretched – allowing time to implement further health measures and protect it from becoming overwhelmed,” Premier Andrews said.
“The Burnet modelling also shows that the key to opening up and reducing risk in Victoria will be making sure workers across the state are vaccinated.”
Modelling the Victorian roadmap
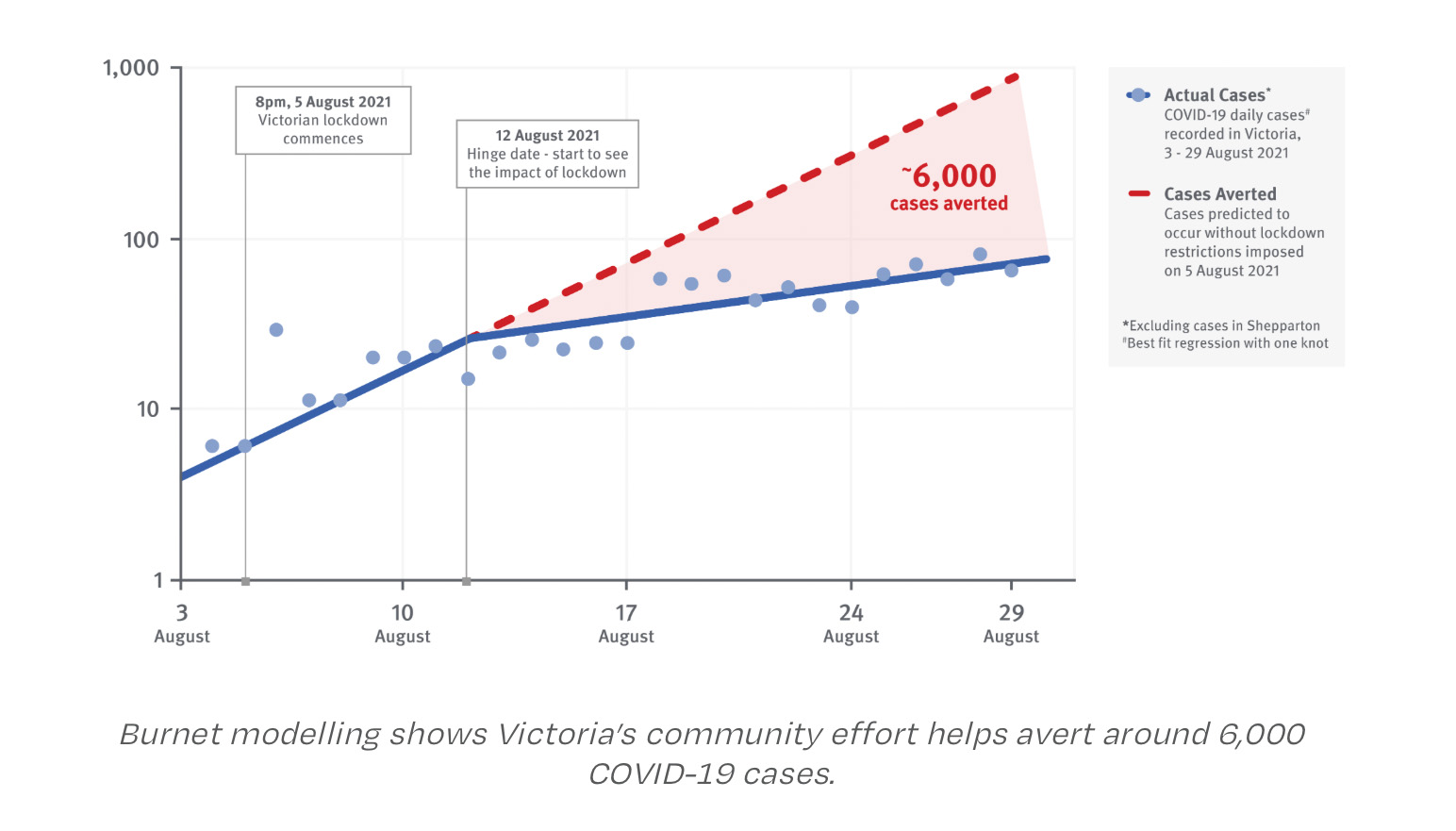
From July 2021 Melbourne experienced a resurgence in delta variant COVID-19 cases. Despite a lockdown being introduced on 5 August, cases continued to grow, and at 17 September daily diagnoses reached a 7-day average of 454.
With Victoria’s COVID-19 strategy shifting away from COVID-zero, protecting the health of the population required achieving high vaccination coverage as quickly as possible, maintaining control of the epidemic to protect the vulnerable, and ensuring that the health system has capacity to provide care to all who need it. An important question was: as vaccine coverage increases, how best can restrictions be eased that prevents health system capacity from being exceeded?
The Covasim model was used to simulate options for easing of restrictions over the October-December period. Model inputs included data on demographics, contact networks, workforce composition, contact tracing systems and age-specific vaccination rates. As well as options for easing restrictions, additional policies around vaccine allocation and testing were examined to determine potential approaches to further reduce the epidemic peak.
Scenarios were run to estimate the number of COVID-19 infections, hospitalisations and ICU requirements in Melbourne:
- Maintained lockdown: A counterfactual scenario to set baseline estimates from which restrictions are eased.
- Roadmap: School and childcare returned throughout October; increased outdoor activities at 70% two-dose vaccine coverage (people 16+ years); retail and indoor activities with density limits commenced at 80% adult vaccine coverage; and mandatory vaccination of authorised workers, teachers, childcare workers, parents of children in childcare, hospitality workers, hospitality patrons.
- Roadmap with additional testing: The roadmap scenario but assuming vaccinated people continue to seek symptomatic testing at the same rate as non-vaccinated people, even for mild symptoms.
- Roadmap with a 15% reduction in non-household transmission. The roadmap scenario, but with an assumption that a 15% reduction in non-household transmission could be achieved immediately and sustained.
Easing stage 4 restrictions in 2020
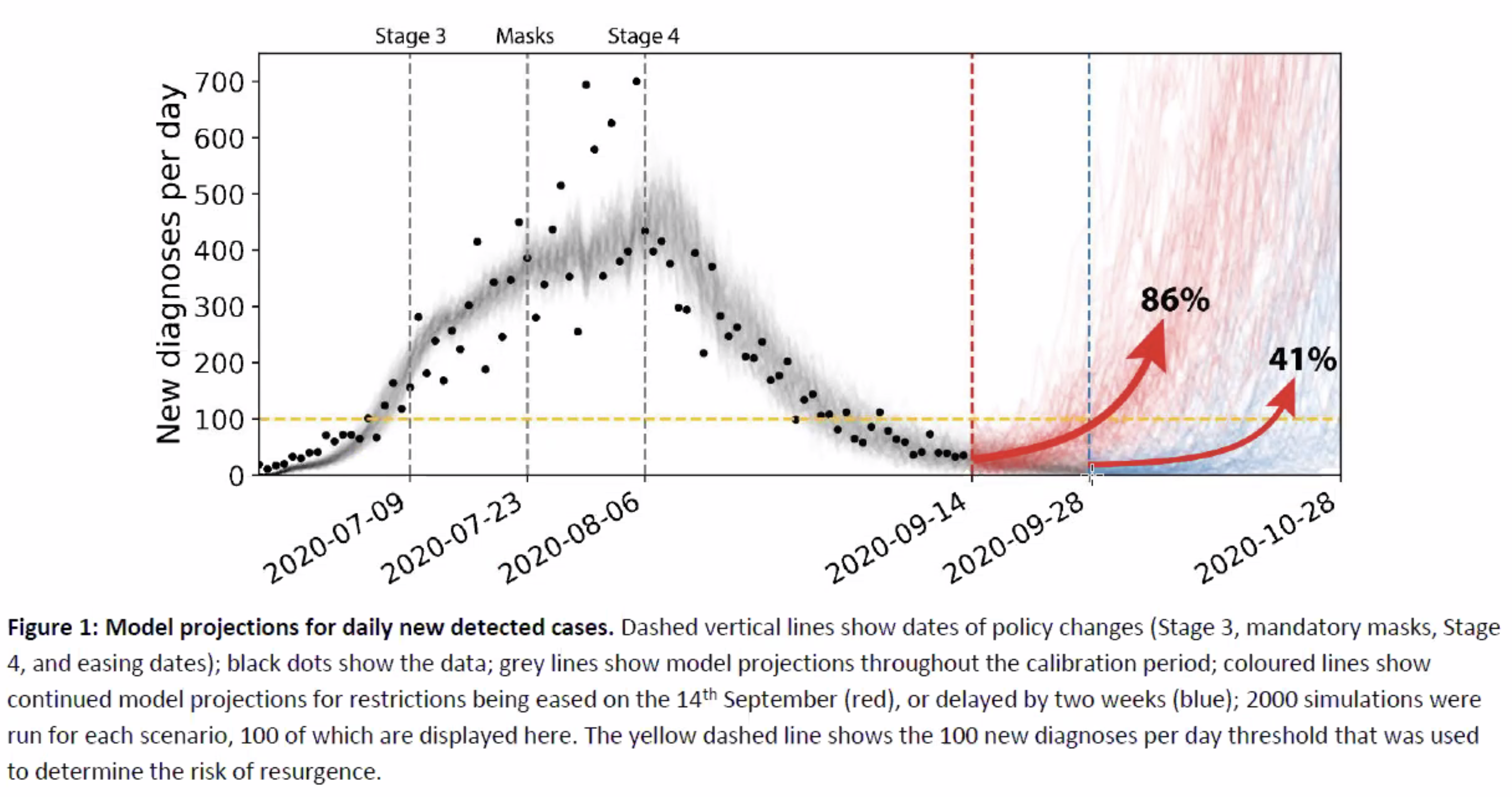
Following the introduction of Stage 4 restrictions in Melbourne in 2020, daily new detected cases of COVID-19 had been declining. Accordingly, a roadmap detailing possible sequences of policy relaxations was been proposed to return to a “COVID normal”, together with criteria for triggering each step. Due to the high social and economic impact of the restrictions currently in place, it was important that restrictions be relaxed as quickly as possible. However, relaxing too quickly increases the risk of a resurgence in infections, which may then require a reintroduction of restrictions to contain.
In this study, we used Covasim to estimate the risk of Victoria experiencing a resurgence in COVID-19 if Stage 4 restrictions were eased on the 14th September 2020 or two weeks later on the 28th September.
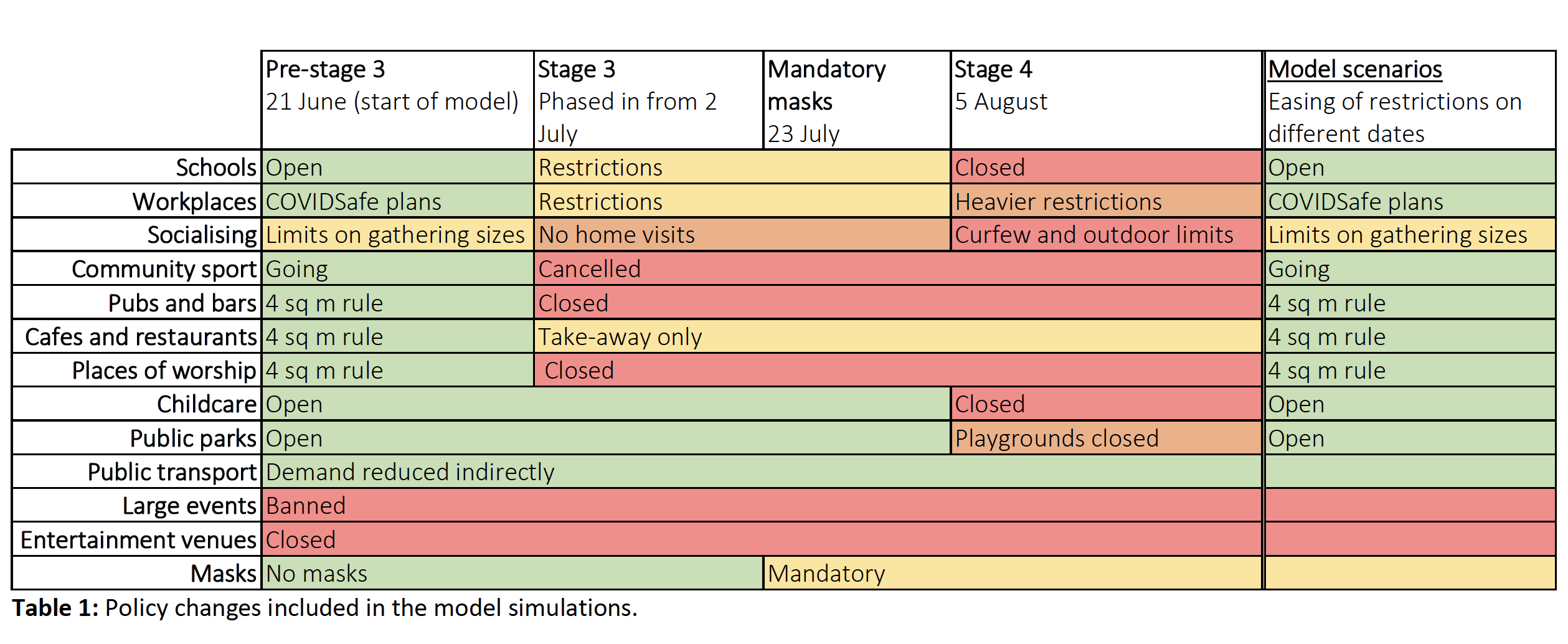
In both scenarios, restrictions were eased to a level of restrictions similar to Victoria in early June 2020 (pre-Stage 3), approximately the “final step” in the Victorian government roadmap or NSW in September. Specifically we modelled:
- Schools, childcare and workplaces reopen
- Cafes, restaurants, pubs, bars, entertainment venues, and places of worship all open with a four square metre distancing rule
- Community sport and small social gatherings are allowed
- Test results take 24 hours to become available
- Contact tracing takes an additional 24 hours following test results, and includes use of the COVIDSafe app
- The number of tests per day is increased to maximum capacity observed in June upon easing
- Large events are banned and mandatory masks are maintained.
While there are a wide range of options for incremental relaxation, in this study we sought to specifically examine the impact of timing, to examine the relationship between the degree of containment prior to relaxation and resurgence risk.
Easing restrictions during vaccination campaigns
Model scenarios were run, calibrated to Victoria, Australia, to help answer the question: What is the impact of different levels of vaccine coverage, if public health control measures were stopped and the virus was allowed to spread through the community?
Burnet Institute has developed an Excel-based tool that summarises thousands of simulations of different scenarios. In each scenario, new infections (one per day) begin to be introduced to the Victorian community at some point following the commencement of vaccine rollout. The vaccine rollout is assumed to continue at a fixed rate with increasing coverage every week.
The tool can compare outcomes when different COVID-19 strains are introduced, and vaccine efficacy assumptions are varied. Before using the tool or interpreting outcomes it is critical that the following key points and examples are read and understood. For additional information, or advice in interpretations, please contact the authors.
Critical points for understanding these projections
- The scenarios assume a user-defined vaccine rollout speed of either 150,000 or 250,000 doses per week in Victoria (75,000 or 125,000 vaccinated people per week, due to second doses). The results are different if the rate of vaccine rollout is different.
- The scenarios do not currently include any major public health response to gain control of outbreaks. On detection of the first case, the model assumes symptomatic testing increases (isolation of positive cases continues), masks become recommended but not mandatory, and contact tracing continues but only up to 250 diagnoses per day. Hence the projections represent hypothetical near-worst-case scenarios.
- The results are based on a collection of model assumptions about the contacts of individuals and disease transmission dynamics . If these best-estimate assumptions are optimistic or pessimistic, then compared with these projections actual epidemic outcomes will be more optimistic or pessimistic respectively.
- One scenario created by Burnet Institute Head of Modelling, Dr Nick Scott and colleagues assumed a 50 per cent vaccine efficacy in preventing infections and a 93 per cent efficacy at preventing deaths among people who did become infected; a virus which was 1.5 times as infectious as the one in Victoria in June-November 2020; and where 80 per cent of people aged over 60 and 70 per cent of people younger than 60 years of age were eventually vaccinated.
“We found that if the virus enters the community when 60 per cent vaccine coverage has been reached and is left unchecked, we could see 4,885 deaths in Victoria within a year if no public health responses are introduced,” Dr Scott said.
“If we get peak vaccination coverage up to 95 per cent, the number of deaths reduces to 1346.”
Conclusions and Recommendations
- Vaccine hesitancy and the emergence of new COVID-19 variants mean Australia is unlikely to achieve herd immunity
- Public health initiatives remain vital in controlling COVID-19, even in vaccinated populations. Without public health measures, thousands of Victorians would be hospitalised and die if an initially small outbreak was left to spread through the community unchecked
- Australia would require higher vaccine coverage to return to normal life.
Visit the Know-C19 Hub for more policy briefs and reports from the Know-C19 team.
Project
Team
Meet the project team. Together, we are translating research into better health, for all.












Publications
VIEW ALL RESEARCHKerr CC, Stuart RM, Mistry D, Abeysuriya RG, Rosenfeld K, Hart GR, Núñez RC, Cohen JA, Selvaraj P, Hagedorn B, George L, Jastrzębski M, Izzo AS, Fowler G, Palmer A, Delport D, Scott N, Kelly SL, Bennette CS, Wagner BG, Chang ST, Oron AP, Wenger EA, Panovska-Griffiths J, Famulare M, Klein DJ
- PLoS Computational Biology
- 26 Jul 2021

Scott N, Palmer A, Delport D, Abeysuriya R, Stuart RM, Kerr CC, Mistry D, Klein DJ, Sacks-Davis R, Heath K, Hainsworth SW, Pedrana A, Stoove M, Wilson D, Hellard ME
- The Medical Journal of Australia
- 18 Nov 2020
Abeysuriya RG, Delport D, Stuart RM, Sacks-Davis R, Kerr CC, Mistry D, Klein DJ, Hellard M, Scott N
- BMC Infect Dis
- 07 Mar 2022
Stuart RM, Abeysuriya RG, Kerr CC, Mistry D, Klein DJ, Gray RT, Hellard M, Scott N
- BMJ Open
- 20 Apr 2021
Houdroge F, Palmer A, Delport D, Walsh T, Kelly SL, Hainsworth SW, Abeysuriya R, Stuart RM, Kerr CC, Coplan P, Wilson DP, Scott N
- Scientific Reports
- 25 Jan 2023